After years of uncontrolled hypertension despite combination antihypertensive therapy, along with unexplained hypokalemia, a Filipino patient was diagnosed with primary aldosteronism secondary to an adrenal adenoma - a potentially dangerous endocrine disorder that frequently goes undetected.
A 30-Year struggle to identify the cause of uncontrolled hypertension
L.C., a 61-year-old man from the Philippines, sought medical care at Hong Ngoc General Hospital - Phuc Truong Minh with a blood pressure of 160/100 mmHg. He reported a more than 30-year history of hypertension and over two decades of persistent hypokalemia, for which no definitive cause had ever been established.
Although he had been prescribed multiple antihypertensive agents, his blood pressure continued to fluctuate and remained difficult to control.
Further review of the patient's medical history revealed a previous cerebral infarction, adding complexity to both the diagnostic evaluation and treatment strategy.
Suspecting secondary hypertension associated with an underlying endocrine disorder, physicians from the Department of Endocrinology at Hong Ngoc General Hospital ordered a series of specialized investigations.
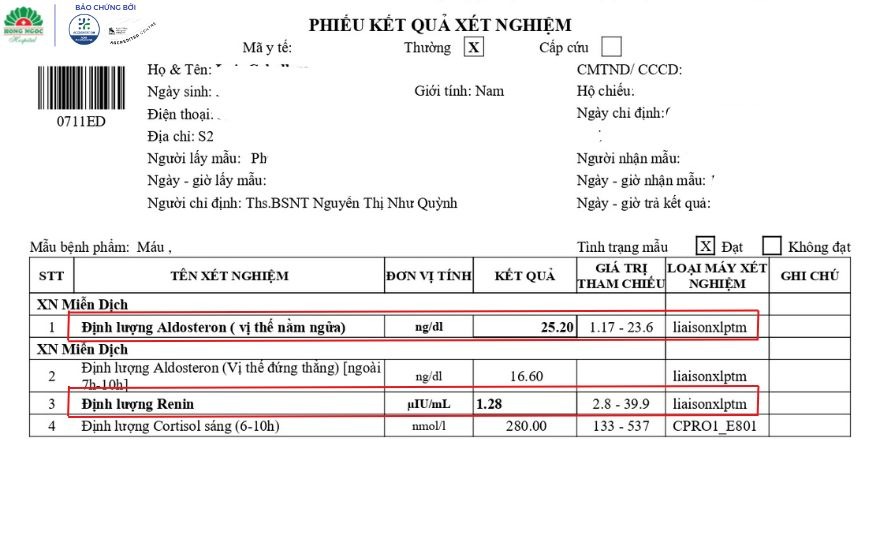
Endocrine testing revealed that aldosterone, a hormone responsible for regulating sodium and water retention, was nearly three times above the normal range. In contrast, renin, a key hormone involved in blood pressure regulation and fluid-electrolyte balance, was markedly suppressed, measuring only about one-third of the lower limit of normal. At the same time, the patient's serum potassium level had fallen to 2.92 mmol/L, significantly below the normal range.
Endocrine testing revealed a markedly elevated aldosterone-to-renin ratio.
The combination of a markedly elevated aldosterone-to-renin ratio (ARR) and persistent hypokalemia met the diagnostic criteria for primary aldosteronism, an endocrine disorder that can lead to resistant hypertension and significantly increase the risk of complications such as stroke and heart attack.
Primary Aldosteronism: The hidden culprit behind decades of hypertension
Primary aldosteronism is a condition in which one or both adrenal glands produce excessive amounts of aldosterone, a hormone responsible for regulating the body's sodium and fluid balance. When aldosterone levels become abnormally elevated, the body retains excess sodium and water while increasing potassium loss through the kidneys, leading to hypertension and hypokalemia.
It is one of the most common causes of secondary hypertension, yet it remains frequently underrecognized and underdiagnosed in clinical practice.
According to Dr. Kieu Hong Nhung, MSc, Resident Physician, Department of Endocrinology, Hong Ngoc General Hospital:
"Many patients receive treatment for hypertension for years without undergoing comprehensive endocrine evaluation, resulting in delayed identification of the underlying cause. Without timely diagnosis and intervention, prolonged excess aldosterone can significantly increase the risk of cardiovascular complications, stroke, and kidney damage."
To further investigate the condition, the patient underwent 2560-slice CT scanning. The imaging revealed bilateral adrenal tumors, with a lesion measuring 8 × 11 mm in the left adrenal gland and another measuring approximately 14 mm in the right adrenal gland.
However, in patients with tumors in both adrenal glands, accurately determining which gland is responsible for excess hormone production is critical in guiding treatment decisions.
To identify the source of aldosterone secretion, the endocrinology team collaborated with interventional radiologists to perform adrenal vein sampling (AVS), a procedure widely regarded as the gold standard for the diagnosis and subtype classification of primary aldosteronism.
The medical team performs adrenal vein sampling (AVS).
According to Dr. Do Huy Hoang, MSc, the interventional radiologist who performed the procedure, adrenal vein sampling (AVS) is a technically challenging procedure. The adrenal veins are extremely small, fragile, and prone to injury, while the right adrenal vein is particularly difficult to access because of its complex anatomy.
Successful catheterization requires exceptional precision and considerable operator experience to obtain accurate diagnostic results.
The AVS procedure was performed by Dr. Do Huy Hoang, MSc, in the interventional radiology suite using a state-of-the-art digital subtraction angiography (DSA) system from the Netherlands. Through a needle puncture measuring only a few millimeters, the physician advanced a microcatheter to precisely access the adrenal vein and obtain blood samples.
The procedure was performed under local anesthesia without the need for general anesthesia, allowing for rapid recovery while maintaining a high level of diagnostic accuracy.
AVS results confirmed that both adrenal glands were producing excessive amounts of aldosterone. The patient was diagnosed with primary aldosteronism caused by bilateral adrenal hyperplasia, the underlying condition responsible for his longstanding hypertension and persistent hypokalemia.
Following confirmation of the diagnosis, the patient was started on targeted medical therapy with a mineralocorticoid receptor antagonist.
After treatment, his blood pressure improved significantly despite a substantial reduction in the number of antihypertensive medications required. His serum potassium levels returned to the normal range, and his overall condition stabilized rapidly.
The patient made a good recovery after four days of treatment.
According to the medical team, integrating advanced endocrine evaluation with specialized interventional techniques is essential for uncovering the underlying causes of persistent hypertension. Accurate diagnosis allows treatment to be directed at the root cause of the condition, rather than focusing solely on symptomatic blood pressure control.
Hong Ngoc General Hospital's Department of Endocrinology delivers specialized screening and treatment for endocrine and metabolic disorders through a high-level clinical care model:
A team of endocrinologists with more than 20 years of experience and advanced training in diabetes, thyroid disorders, and hormonal diseases.
Advanced diagnostic technology, including a 2560-slice CT scanner, Signa MRI system, LOGIQ ultrasound platform, and GLP-compliant automated laboratory systems.
Evidence-based treatment protocols and a comprehensive, patient-centered care pathway aligned with ACHSI international healthcare standards.
Hotline: 0911 858 626Address: 8 Chau Van Liem Street, Tu Liem Ward, Hanoi
After years of uncontrolled hypertension despite combination antihypertensive therapy, along with unexplained hypokalemia, a Filipino patient was diagnosed with primary aldosteronism secondary to an adrenal adenoma - a potentially dangerous endocrine disorder that frequently goes undetected.
A 30-Year struggle to identify the cause of uncontrolled hypertension
L.C., a 61-year-old man from the Philippines, sought medical care at Hong Ngoc General Hospital - Phuc Truong Minh with a blood pressure of 160/100 mmHg. He reported a more than 30-year history of hypertension and over two decades of persistent hypokalemia, for which no definitive cause had ever been established.
Although he had been prescribed multiple antihypertensive agents, his blood pressure continued to fluctuate and remained difficult to control.
Further review of the patient's medical history revealed a previous cerebral infarction, adding complexity to both the diagnostic evaluation and treatment strategy.
Suspecting secondary hypertension associated with an underlying endocrine disorder, physicians from the Department of Endocrinology at Hong Ngoc General Hospital ordered a series of specialized investigations.
Endocrine testing revealed that aldosterone, a hormone responsible for regulating sodium and water retention, was nearly three times above the normal range. In contrast, renin, a key hormone involved in blood pressure regulation and fluid-electrolyte balance, was markedly suppressed, measuring only about one-third of the lower limit of normal. At the same time, the patient's serum potassium level had fallen to 2.92 mmol/L, significantly below the normal range.
Endocrine testing revealed a markedly elevated aldosterone-to-renin ratio.
The combination of a markedly elevated aldosterone-to-renin ratio (ARR) and persistent hypokalemia met the diagnostic criteria for primary aldosteronism, an endocrine disorder that can lead to resistant hypertension and significantly increase the risk of complications such as stroke and heart attack.
Primary Aldosteronism: The hidden culprit behind decades of hypertension
Primary aldosteronism is a condition in which one or both adrenal glands produce excessive amounts of aldosterone, a hormone responsible for regulating the body's sodium and fluid balance. When aldosterone levels become abnormally elevated, the body retains excess sodium and water while increasing potassium loss through the kidneys, leading to hypertension and hypokalemia.
It is one of the most common causes of secondary hypertension, yet it remains frequently underrecognized and underdiagnosed in clinical practice.
According to Dr. Kieu Hong Nhung, MSc, Resident Physician, Department of Endocrinology, Hong Ngoc General Hospital:
"Many patients receive treatment for hypertension for years without undergoing comprehensive endocrine evaluation, resulting in delayed identification of the underlying cause. Without timely diagnosis and intervention, prolonged excess aldosterone can significantly increase the risk of cardiovascular complications, stroke, and kidney damage."
To further investigate the condition, the patient underwent 2560-slice CT scanning. The imaging revealed bilateral adrenal tumors, with a lesion measuring 8 × 11 mm in the left adrenal gland and another measuring approximately 14 mm in the right adrenal gland.
However, in patients with tumors in both adrenal glands, accurately determining which gland is responsible for excess hormone production is critical in guiding treatment decisions.
To identify the source of aldosterone secretion, the endocrinology team collaborated with interventional radiologists to perform adrenal vein sampling (AVS), a procedure widely regarded as the gold standard for the diagnosis and subtype classification of primary aldosteronism.
The medical team performs adrenal vein sampling (AVS).
According to Dr. Do Huy Hoang, MSc, the interventional radiologist who performed the procedure, adrenal vein sampling (AVS) is a technically challenging procedure. The adrenal veins are extremely small, fragile, and prone to injury, while the right adrenal vein is particularly difficult to access because of its complex anatomy.
Successful catheterization requires exceptional precision and considerable operator experience to obtain accurate diagnostic results.
The AVS procedure was performed by Dr. Do Huy Hoang, MSc, in the interventional radiology suite using a state-of-the-art digital subtraction angiography (DSA) system from the Netherlands. Through a needle puncture measuring only a few millimeters, the physician advanced a microcatheter to precisely access the adrenal vein and obtain blood samples.
The procedure was performed under local anesthesia without the need for general anesthesia, allowing for rapid recovery while maintaining a high level of diagnostic accuracy.
AVS results confirmed that both adrenal glands were producing excessive amounts of aldosterone. The patient was diagnosed with primary aldosteronism caused by bilateral adrenal hyperplasia, the underlying condition responsible for his longstanding hypertension and persistent hypokalemia.
Following confirmation of the diagnosis, the patient was started on targeted medical therapy with a mineralocorticoid receptor antagonist.
After treatment, his blood pressure improved significantly despite a substantial reduction in the number of antihypertensive medications required. His serum potassium levels returned to the normal range, and his overall condition stabilized rapidly.
The patient made a good recovery after four days of treatment.
According to the medical team, integrating advanced endocrine evaluation with specialized interventional techniques is essential for uncovering the underlying causes of persistent hypertension. Accurate diagnosis allows treatment to be directed at the root cause of the condition, rather than focusing solely on symptomatic blood pressure control.
Hong Ngoc General Hospital's Department of Endocrinology delivers specialized screening and treatment for endocrine and metabolic disorders through a high-level clinical care model:
A team of endocrinologists with more than 20 years of experience and advanced training in diabetes, thyroid disorders, and hormonal diseases.
Advanced diagnostic technology, including a 2560-slice CT scanner, Signa MRI system, LOGIQ ultrasound platform, and GLP-compliant automated laboratory systems.
Evidence-based treatment protocols and a comprehensive, patient-centered care pathway aligned with ACHSI international healthcare standards.
Hotline: 0911 858 626Address: 8 Chau Van Liem Street, Tu Liem Ward, Hanoi
Để lại câu hỏi của bạn để nhận được giải đáp từ các bác sĩ của Hồng Ngọc
Lorem ipsum dolor
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Mauris odio lectus, pretium faucibus nisi eu, accumsan consectetur orci. In blandit vehicula nisl, vel lacinia ligula finibus a. Donec fermentum rhoncus
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Mauris odio lectus, pretium faucibus nisi eu, accumsan consectetur orci. In blandit vehicula nisl, vel lacinia ligula finibus a. Donec fermentum rhoncus
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Mauris odio lectus, pretium faucibus nisi eu, accumsan consectetur orci. In blandit vehicula nisl, vel lacinia ligula finibus a. Donec fermentum rhoncus
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Mauris odio lectus, pretium faucibus nisi eu, accumsan consectetur orci. In blandit vehicula nisl, vel lacinia ligula finibus a. Donec fermentum rhoncus
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Mauris odio lectus, pretium faucibus nisi eu, accumsan consectetur orci. In blandit vehicula nisl, vel lacinia ligula finibus a. Donec fermentum rhoncus